

_Clare Milner
Milner is an associated professor in the Department of Physical Therapy and Rehabilitation Sciences in the College of Nursing and Health Professions and a fellow of the American College of Sports Medicine.
Running is one of the most convenient forms of exercise available — it’s cheap, you can do it practically anywhere, year-round, and there is no heavy equipment needed, or membership required. Small wonder attendance at races and marathons has soared in recent years.
But alongside this list of “pros,” is a serious “con” demanding attention: the high risk of injury.
“It’s the same idea as coaching a pitcher: It’s expected you‘ll be coached on your pitching technique. We are interested in training a runner to alter their running technique if they have aberrant biomechanics, as a way to avoid or reduce the risk of those injuries.”
—Clare Milner,
associate professor in the College of Nursing
and Health Professions
Running injuries are fairly common — in an average mile-long course, a runner makes impact with the ground about 1,500 times. Multiply that by the length of a 26-mile marathon and that’s 39,000 opportunities for something to go wrong. By one estimate, if 10 friends were to start a new running group, five to seven of them would be injured within a year. The most typical running problems, called overuse injuries, range from tibial stress fractures (sometimes called shin splints), patellofemoral pain (pain behind the kneecap) and plantar fasciitis (pain in the heel).
Yet while running has rapidly gained new converts, the science of running and rehabilitation is racing to catch up.
At Drexel University, rehabilitation scientists are now working alongside each other in a new facility to understand how injuries happen and help injured runners get back in the race. Introduced last fall, the University’s new state-of-the-art College of Nursing and Health Professions facility combines researchers and clinical resources (called Parkway Health & Wellness) in 23,000 square feet in Center City.
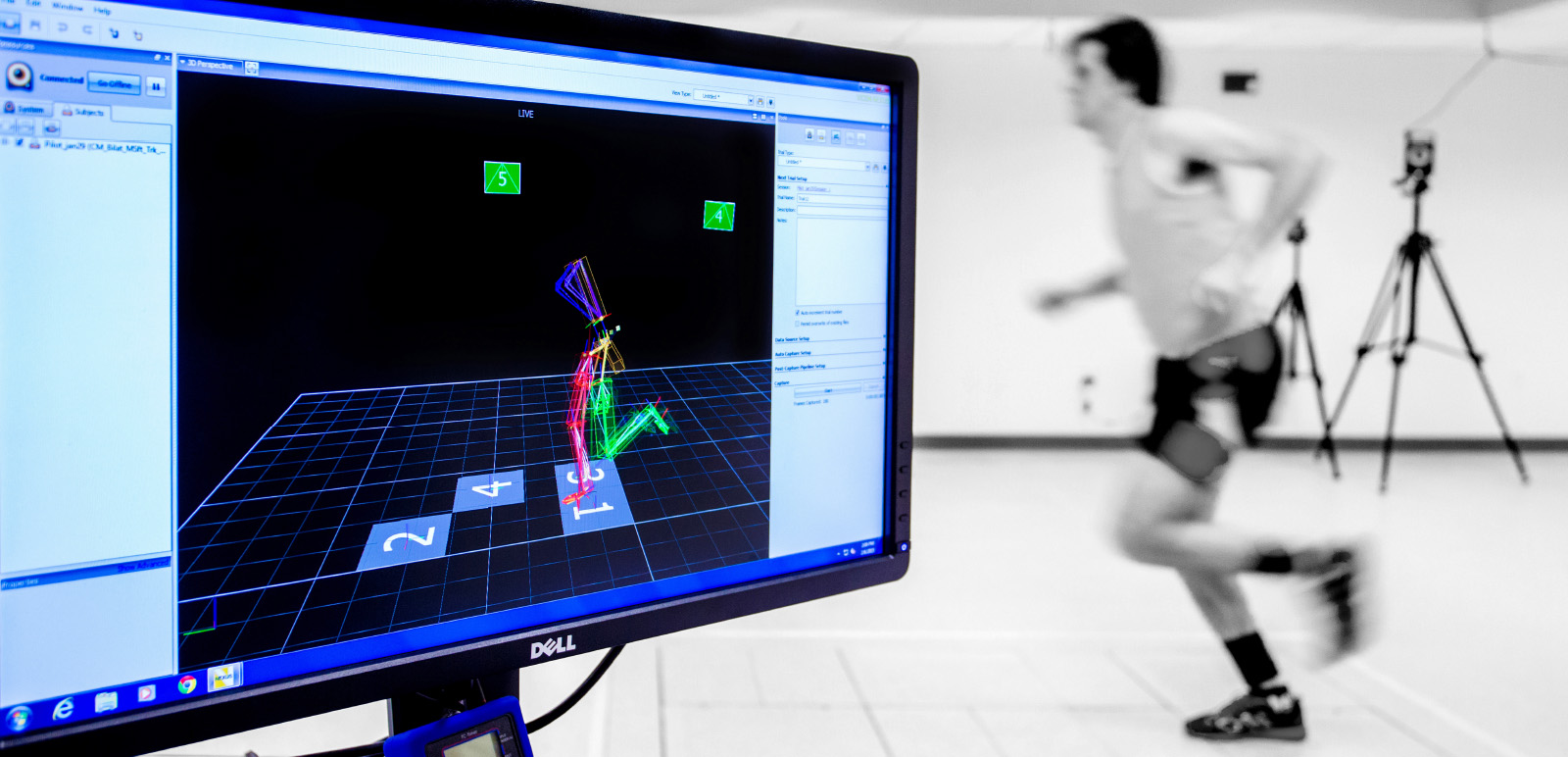
One highlight of the site’s research capabilities is a windowless room equipped with high-tech sensing equipment and cameras, called the Gait Lab.
Here, research participants don running shorts and special tracking markers and practice dashing across a group of sensing plates embedded in the floor, while cameras and a nearby computer monitor tracks and analyzes their movements.
The room is the setting for a number of studies related to running, including one that examines “foot strike pattern” and its link to overuse injuries.
Foot strike pattern refers to how or where a runner’s foot strikes the ground. It has become a buzzword in running circles in recent years because of the popularity (or notoriety) of barefoot running and “minimalist” shoes — a trend pioneered by Vibram’s line of FiveFingers glove-like footwear.
Runners raced to buy Vibram’s shoes on the promise of a barefoot-like experience that protected feet from injuries and strengthened running muscles. But the company had no scientific data to back it up, and last year Vibram agreed to pay out $3.75 million to past customers to settle a class-action suit that alleged that the company made false health claims.
If nothing else, the lawsuit shines a spotlight on the dearth of research in this area.
One of the studies underway in the Gait Lab takes the barefoot/shod debate out of the equation and studies runners’ movement to better understand the mechanics of overuse injuries. For example, if you naturally land with your heel first (rearfoot strike), you might be more likely to develop bony injuries such as tibial stress fractures.
nimble_science
The Gait Lab inside Drexel’s new College of Nursing and Health Professions facility is equipped with cameras and wearable markers to help researchers study
running movements and foot strike patterns.
Clare Milner, the associate professor in the College of Nursing and Health Professions who heads the study, is focusing on how foot strike differences between men and women play into the types of injuries they experience.
“Men and women get injured at different rates, and often with different injuries — female runners are more likely to get Iliotibial band syndrome (pain on the side of the knee), and male runners get Achilles tendinitis more often, for example,” she says.
The goal of the study, Milner says, is to eventually develop some evidence-based rehabilitation.
Milner and colleagues call it “gait retraining.”
“We want to modify the way a person runs to get them into a pattern that is going to protect them from those injuries,” Milner says. “It’s the same idea as coaching a pitcher: It’s expected you‘ll be coached on your pitching technique. We are interested in training a runner to alter their running technique if they have aberrant biomechanics, as a way to avoid or reduce the risk of those injuries.”
Some studies have shown that a rearfoot striker may experience less impact on the lower extremities by switching to a forefoot strike, or landing more on the ball of the foot.
But Milner points out that while preliminary results show less impact with a forefoot strike, there really is no universally “right” foot strike.
“Nothing is that simple,” she says. “That’s why we really wanted to dig into this.”
In the Gait Lab, Milner performs a gait analysis using the room’s system of sensing equipment and recording software. The lab is equipped with numerous cameras to record a runner’s movement. Exactly 68 reflective tracker balls are attached to the subject at key anatomical points: the foot, knee, trunk, etc. As the study participant runs through the center of the room, he or she passes through a circle rimmed by eight cameras that detect the trackers and capture his or her running biomechanics. Force plates hidden in the floor measure the ground-reaction force when the runner strikes the ground.
Together, these tools and accompanying software provide a 3-D picture of a subject’s joint torque and movement for the lower extremity joints.
The study is currently in its data crunch phase, and Milner and her team are realizing there actually is a “right” way to run, or at least a “better” way, in order to avoid injury. The catch is that it’s different for every individual; the one-size-fits-all approach to treatment just won’t work.
“It’s really just a matter of teaching people to run in the way that’s best for them so they can stay with their active lifestyle,” Milner says.
By consulting with physical therapists who operate in the same building, runners can make changes to their form to keep them going strong, prevent future injuries and even improve their performance. Changes can include altering one’s foot strike pattern, or making changes to one’s step width and step length.
For Kelly Shaffer, a 17-year-old high school junior who runs track, a short visit with a physical therapist at Parkway Health & Wellness was enough to keep her on her feet.
When her spring track season last year was cut short because of painful shin splints, her athletic trainer referred her to Drexel’s Robert Maschi, an assistant clinical professor and expert in gait retraining who operates a runner’s clinic out of the same facility that houses the Gait Lab.
In Maschi’s clinic, runners’ movements are monitored from multiple angles by video that is then subjected to a two-dimensional motion analysis.
“From the video, we can assess for movement patterns that may put the runner at increased risk for injury,” says Maschi. “This involves looking at stride length, stride width, foot strike pattern and total amount of movement at all joints during running. Using this information in combination with the client’s running history and musculoskeletal exam, we can make recommendations regarding gait modification, exercise intervention, change in shoes or orthotic inserts and training plan.”
“It was just one afternoon, for about an hour or so; Dr. Maschi had me run on the treadmill and complete some other strength tests,” Shaffer says. “The primary thing he said for me to do was not to heel strike. He recommended I change my cadence in order to do that. And now I’m a mid-foot striker.”
The small adjustment made a big impact.
“The problem didn’t go away completely, but I think it did make it better,” she says. “I have less pain and it helped me put off actually having a stress fracture. And,” she proudly adds, “I was able to finish the whole cross-country season.”